Comprehensive large-scale hypertension program greatly improves hypertension control rate
21/08/2013
A community-based hypertension program encompassing a registry, active monitoring of performance, guidelines, and single-pill combination pharmacotherapy was effective at improving hypertension control.
Improved Blood Pressure Control Associated With a Large-Scale Hypertension ProgramLiterature - Jaffe MG, Lee GA, Young JD et al. - JAMA. 2013;310(7):699-705
Jaffe MG, Lee GA, Young JD et al.
JAMA. 2013;310(7):699-705. doi:10.1001/jama.2013.108769
Background
Fewer than half of hypertensive Americans had controlled blood pressure in 2001-2002 [1]. Thus far, no successful long-term large-scale programme has been described. A review of 72 clinical trials has identified several interventions that can improve blood pressure control in primary care settings [2].Kaiser Permanente Northern California (KPNC) a not-for-profit integrated health care delivery system caring for over 2.3 million adults. Comprehensive inpatient and outpatient care is provided through 21 hospitals, 45 medical facilities, and over 7000 physicians. A multifaceted quality improvement program for hypertension was developed by KPNC in 2001. This paper describes its results for the period between 2001 and 2009. (for details on the development and implementation of the program, we refer to the original article).
Main results
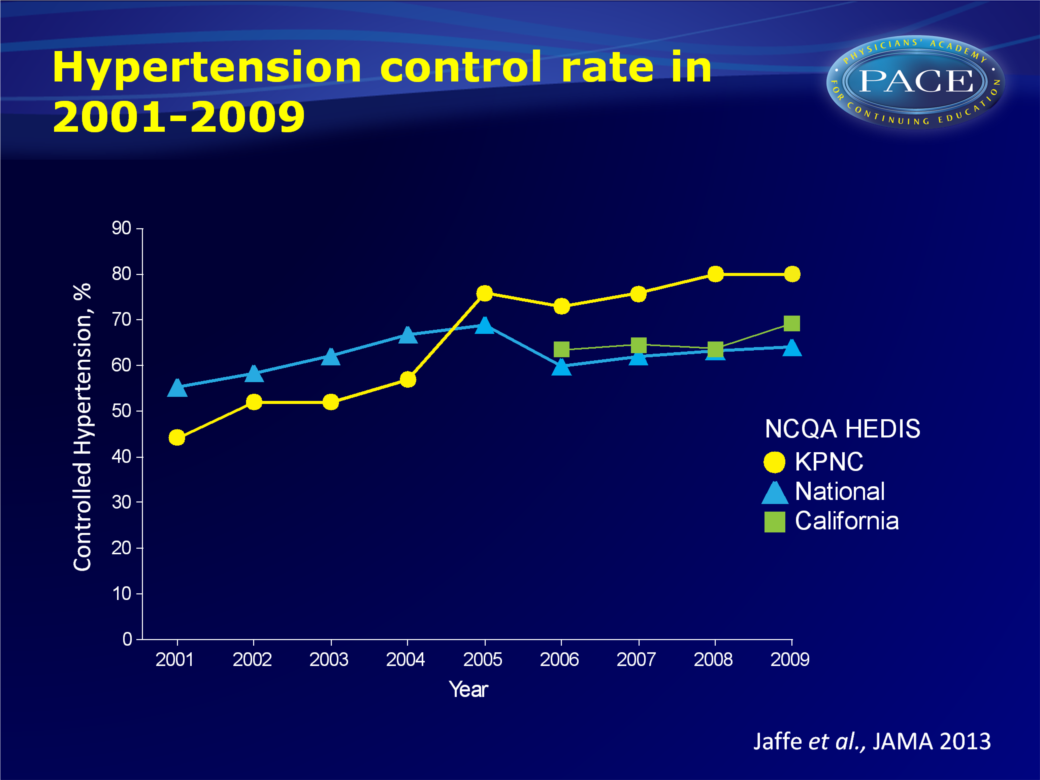
- After implementation of the hypertension program, commercial hypertension control (according to the National Committee for Quality Assurance (NCQA) Healthcare Effectiveness Data and Information Set (HEDIS) specifications) rate had increased from 43.6% (95%CI: 39.4-48.6) in 2001 to 80.4% (95%CI: 75.6-84.4%) in 2009 (P<0.001 for trend).
In contrast, the national mean NCQA HEDIS control rate increased nonsignificantly from 55.4% to 64.1% in this period, and available data on California (2006 onwards) were slightly higher than the national average (63.4% to 69.4% for 2006 to 2009).
- NCQA HEDIS hypertension control rate in KPNC continued to increase after the study period, from 83.7% in 2010 to 87.1% in 2011.
- During the study period, in which prescription of single-pill combination (SPC) was promoted, lisinopril-hydrochlorothiazide SPC prescriptions increased from 13 to 23144 prescriptions per month. Also ACE-inhibitors in combination with a thiazide diuretic, dispensed as an SPC, were prescribed much more, from less than 1% in 2001 to 27.2%.
Click to download image
Conclusion
This large-scale multifactorial community-based hypertension program nearly doubled hypertension control between 2001 and 2009, a trend not seen on a state- or national level. Key elements of the program include establishment of a comprehensive hypertension registry, development and sharing of performance metrics, evidence-based guidelines, medical assistant visits for blood pressure measurement, and SPC pharmacotherapy.References
1. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988-2008. JAMA. 2010;303(20):2043-2050.
2. Glynn LG, Murphy AW, Smith SM, et al. Interventions used to improve control of blood pressure in patients with hypertension.Cochrane Database Syst Rev. 2010;(3):CD005182.