Larger increase in fibrous cap thickness in atherosclerotic plaque with higher dose statin
Treatment with atorvastatin may stabilise coronary plaques by increasing fibrous cap thickness and decreasing the amount of atherosclerotic plaque, possibly via its anti-inflammatory properties.
BackgroundLiterature - Komukai K et al., JACC 2014
Effect of Atorvastatin Therapy on Fibrous Cap Thickness in Coronary Atherosclerotic Plaque as Assessed by Optical Coherence Tomography: The EASY-FIT Study
Komukai K, Kubo T, Kitabata H et al.,
J Am Coll Cardiol. 2014 Dec 2;64(21):2207-17
Progression of atherosclerosis has been shown to be attenuated by statin therapy [1-3]. More precisely, angioscopy studies demonstrated that statins decreased plaque yellow score, which may reflect the lipid content of coronary plaques [4]. The precise mechanism of how statins stabilise plaques is, however, unclear.
Plaques can be characterised with intravascular optical coherence tomography (ICT) with high resolution [5]. Fibrous cap thickness can be measured, postulated to be in important factor in plaque vulnerability.
The EASY-FIT (Effect of AtorvaStatin therapY on FIbrous cap Thickness in coronary atherosclerotic plaque as assessed by optical coherence tomography) study was a prospective, randomised OCT study in Japan, which evaluated the effect of atorvastatin 20 mg/day (the highest approved dose in Japan) vs. 5 mg/day (standard dose) on fibrous cap thickness in coronary atherosclerotic plaque. Successful OCT at baseline and follow-up was performed in 60 patients with successful percutaneous coronary intervention (PCI) for unstable angina pectoris and untreated dyslipidaemia. The target lesion for OCT was a non-culprit lesion in the PCI-treated artery. Median follow-up time was 12.0 months (IQR: 11.6-12.2 months) in those randomised to 20 mg/day and 11.9 months (IQR: 11.3-12.4) in those receiving 5 mg/day of atorvastatin. No cardiac death or myocardial infarction occurred.
Main results
- The percentage decrease in serum LDL-c was significantly greater in those receiving atorvastatin 20 mg/day than those on 5 mg/day (-46%, IQR: -56% to -39%, vs. -38%, IQR: -47% to -23%, P=0.009).
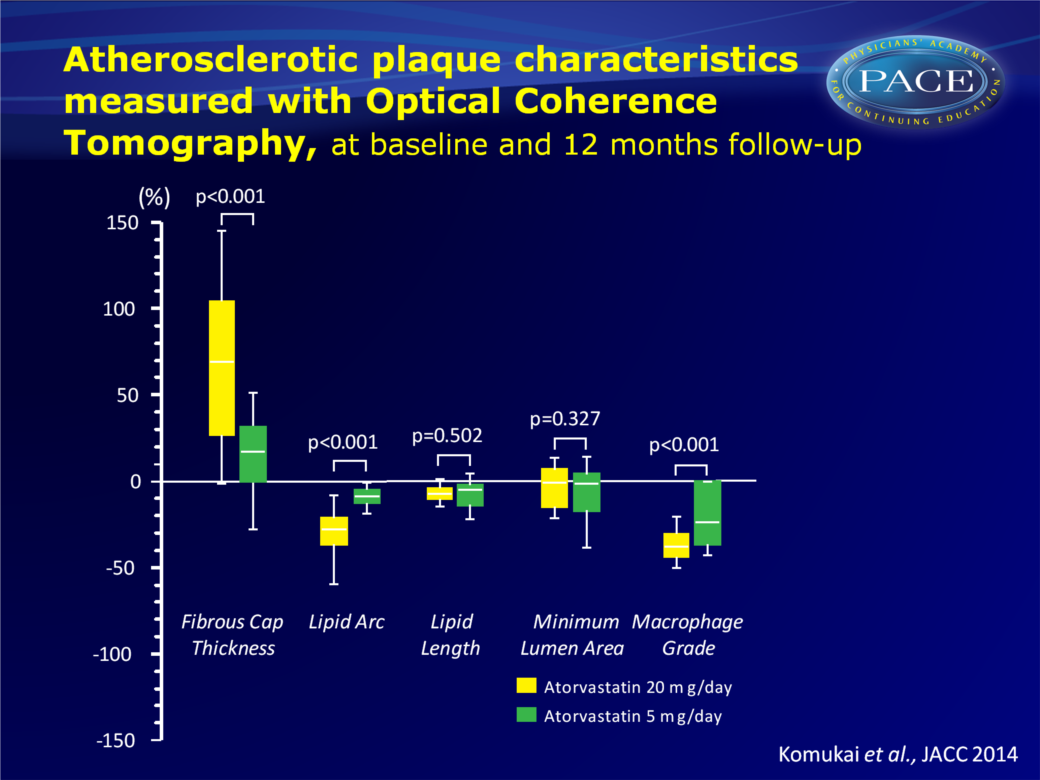
- Fibrous cap thickness increased significantly in both groups, but more so in the group randomised to 20 mg/day (69%, IQR: 25-104%) than those receiving 5 mg/day (17%, IQR: -1% vs. 34%, P<0.001).
- The lipid arc decreased significantly in both groups (20 mg/day: -27%, IQR: -37 to -20%, vs. 5 mg/day: -8%, IQR: -13 to -4%, P<0.001).
- The percentage of plaques with macrophage accumulation at baseline was similar in both groups, and no plaques were seen that newly acquired or were absolutely depleted of macrophages at follow-up. Macrophage grade did decrease significantly in both groups, but to a larger extent in the 20 mg/day group (-38%, IQR: -44 to -31% vs. -24%, IQR: -33% to 0%, P<0.001).
- The percentage change in fibrous cap thickness was significantly negatively correlated with %change in serum LDL-c, MDA-LDL, hs-CRP and MMP-9, but not with %change in total cholesterol, HDL-c, triglyceride, IL-6 and HbA1c.
- The %change in macrophage grade was negatively correlated with %change in serum HDL-c, and positively correlated with serum hs-CRP and MMP-9 levels, but not with the other biomarkers. %Change in macrophage grade also negatively correlated with the %change in fibrous cap thickness.
Conclusion
Therapy with atorvastatin 20 mg/day yielded in a larger increase in fibrous cap thickness and a decrease in lipid arc and macrophage grade than did 5 mg/day. The increased thickness of the fibrous cap was associated with a decrease of unfavourable biomarkers. This study suggests that treatment with atorvastatin 20 mg/day may stabilise coronary atherosclerotic plaques more so than 5 mg/day.Find this article on Pubmed
References
1. Nissen SE, Tuzcu EM, Schoenhagen P, et al. Effect of intensive compared with moderate lipid lowering therapy on progression of coronary atherosclerosis. A randomized controlled trial.JAMA 2004;291:1071–80.
2. Okazaki S, Yokoyama T, Miyauchi K, et al. Early statin treatment in patients with acute coronarysyndrome: demonstration of the beneficial effect on atherosclerotic lesions by serial volumetric intravascular ultrasound analysis during half a year after coronary event: the ESTABLISH Study.Circulation 2004;110:1061–8.
3. Hiro T, Kimura T, Morimoto T, et al. Effect of intensive statin therapy on regression of coronaryatherosclerosis in patients with acute coronary syndrome. A multicenter randomized trial evaluated by volumetric intravascular ultrasound using pitavastatin versus atorvastatin (JAPAN-ACS [Japan Assessment of Pitavastatin and Atorvastatin in Acute Coronary Syndrome] Study) Clinical Trials. J Am Coll Cardiol 2009;54:293–302.
4. Takano M, Mizuno K, Yokoyama S, et al. Changes in coronary plaque color and morphology by lipid-lowering therapy with atorvastatin: serial evaluation by coronary angioscopy. J Am Coll Cardiol 2003;42:680–6.
5. Tearney GJ, Regar E, Akasaka T, et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the international working group for intravascular optical coherence tomography standardization and validation. J Am Coll Cardiol 2012;59:1058–72.