Linagliptin safely improves glycaemic control in elderly patients with T2DM
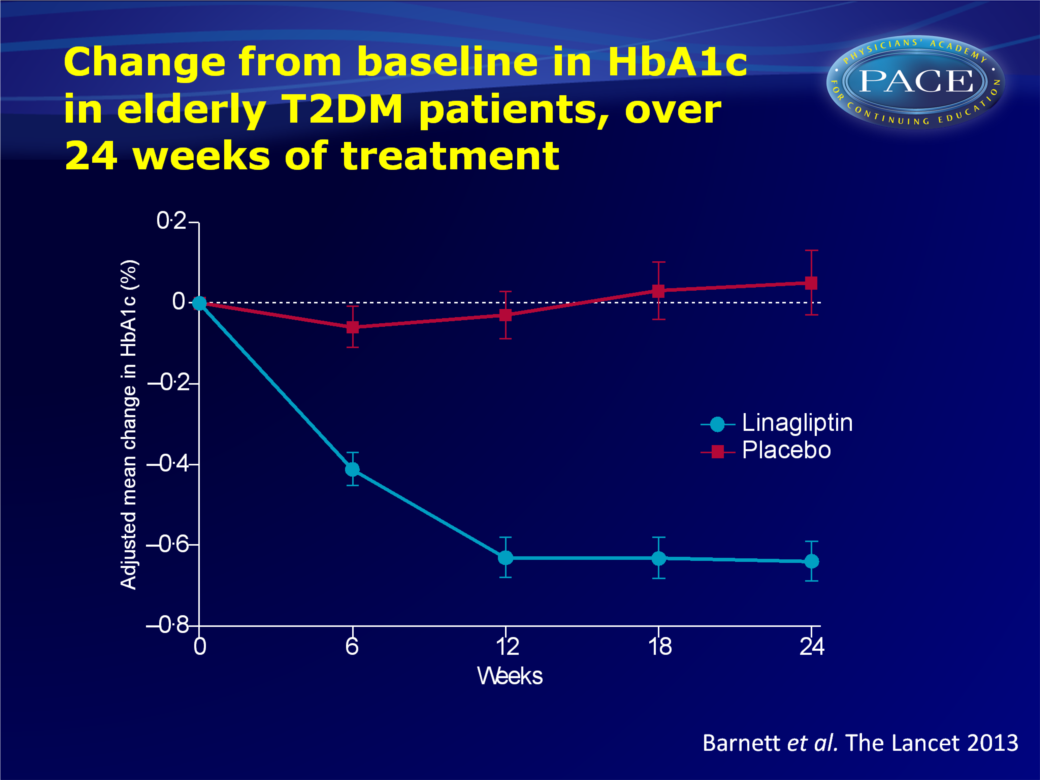
24 weeks of treatment with linagliptin 5 mg gave a clinically meaningful decrease of HbA1c in patients >70 years old, independent of age, duration of disease, renal function and concomitant therapy.
Linagliptin for patients aged 70 years or older with type 2 diabetes inadequately controlled with common antidiabetes treatments: a randomised, double-blind, placebo-controlled trial.Literature - Barnett AH, Huisman H, Jones R, et al. - Lancet. 2013 Aug 12
Barnett AH, Huisman H, Jones R, et al.
Lancet. 2013 Aug 12. doi: 10.1016/S0140-6736(13)61500-7
Background
Although elderly people (>65 years) form a substantial proportion of people with type 2 diabetes mellitus (T2DM), this age category is largely underrepresented in clinical studies [1]. Information is specifically lacking on glucose-lowering treatments in elderly patients with T2DM whose hyperglycaemia is uncontrolled by common antidiabetes treatments [2]. Risks and benefits of these treatments in elderly patients are unclear.Treatment of elderly patients with T2DM is challenging due to frequent comorbidities, polypharmacy, frailty and age-related reduction in pancreatic islet function [3]. Iatrogenic hypoglycaemia can have severe consequences and should be avoided [2,4]. Targets such as HbA1c should be assessed for each individual patient, to balance potential benefits and risks of treatment [2,3,5].
Dipeptidyl peptidase-4 (DDP4) inhibitors are oral agents with little risk for hypoglycaemia [6]. Linagliptin is a DPP4-inhibitors that is mainly excreted by non-renal pathways, thus dose-adjustment is not needed for renal impairment [7]. Linagliptin also has shown minimal drug interactions. Phase III studies have demonstrated that linagliptin had meaningful glucose-lowering effects, with a low intrinsic risk for hypoglycaemia [8-12]. Linagliptin may therefore be particularly useful for treatment of elderly patients with T2DM. This randomised, double-blind, placebo-controlled study therefore tested efficacy, safety and tolerability of linagliptin 5 mg in patients of >70 years old with T2DM with inadequate glycaemic control on other common glucose-lowering drugs (linagliptin: n=160, placebo: n=78).
Main results
- After 24 weeks of treatment, the placebo-adjusted mean change in HbA1c from baseline was -0.64% (95%CI: -0.81 to -0.48, P<0.001).
- Patients with baseline HbA1c above 7.0% more often achieved HbA1c below 7.0% in the linagliptin group (38.9%) than in the placebo group (8.3%, OR 8.32, 95%CI: 3.32-20.84, P<0.001).
- Placebo-adjusted mean reduction in fasting plasma glucose from baseline was -1.15 mmol/L (95%CI: -1.68 to -0.62, P<0.001).
- Rescue treatment was less often needed in the linagliptin group (4.4%) than in the placebo group (14.1%, OR: 0.21, 95%CI: 0.07-0.63, P=0.0048).
- Placebo-adjusted mean changes in HbA1c with linagliptin were generally similar among subgroups based on age, duration of diabetes, renal function and concomitant therapy.
- Investigator-defined hypoglycaemia occurred in 24.1% of patients on linagliptin, and in 16.5% of patients on placebo (OR linagliptin vs. placebo: 1.58, 95%CI: 0.78-3.78, P=0.21). This numerical difference was likely due to the higher incidence of patients receiving sulfonylureas in the linagliptin group (30.5% vs. 16.3% in the placebo group).
Click on image to download
Conclusion
Linagliptin improved glycaemia and was well tolerated in elderly patients with T2DM who had not obtained sufficient glycaemic control with other glucose-lowering drugs. This clinically meaningful effect of linagliptin treatment was independent of age, renal impairment, or diabetes duration. Hypoglycaemia occurred more often only with concomitant treatment with sulfonylureas, thus the latter should be used with caution in the elderly. Thus, in this patient population with advanced disease and many comorborbidites , linagpliptin can be a safe and beneficial addition to existing glucose-lowering drugs.References
1. Lakey WC, Barnard K, Ba tch BC, et al. Are current clinical trials in diabetes addressing important issues in
diabetes care? Diabetologia 2013; 56: 1226–35.
2. Kirkman MS, Briscoe VJ, Clark N, et al. Diabetes in older adults. Diabetes Care 2012; 35: 2650–64.
3. Fravel MA, McDanel DL, Ross MB, et al. Special considerations for treatment of type 2 diabetes mellitus in the elderly. Am J Health Syst Pharm 2011; 68: 500–09.
4. Sinclair A, Morley JE, Rodriguez-Manas L, et al. Diabetes mellitus in older people: position statement on behalf of the International Association of Gerontology and Geriatrics (IAGG), the European Diabetes Working Party for Older People (EDWPOP), and the International Task Force of Experts in Diabetes. J Am Med Dir Assoc
2012; 13: 497–502.
5. Inzucchi SE, Bergenstal RM, Buse JB, et al, and the American Diabetes Association (ADA), and the European Association for the Study of Diabetes (EASD). Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012; 35: 1364–79.
6. Karagiannis T, Paschos P, Paleta s K, et al. Dipeptidyl peptidase-4 inhibitors for treatment of type 2 diabetes
mellitus in the clinical setting: systematic review and meta-analysis. BMJ 2012; 344: e1369.
7. Graefe-Mody U, Retlich S, Friedr ich C. Clinical pharmacokinetics and pharmacodynamics of linagliptin. Clin Pharmacokinet 2012; 51: 411–27.
8. Del Prato S, Barnett AH, Huisman H, et al. Effect of linagliptin monotherapy on glycaemic control and markers of β-cell function in patients with inadequately controlled type 2 diabetes: a randomized controlled trial. Diabetes Obes Metab 2011; 13: 258–67.
9. Gomis R, Espadero RM, Jones R, et al. Effi cacy and safety of initial combination therapy with linagliptin and
pioglitazone in patients with inadequately controlled type 2 diabetes: a randomized, double-blind, placebo-controlled study. Diabetes Obes Metab 2011; 13: 653–61.
10. Taskinen MR, Rosenstock J, Tammine n I, et al. Safety and efficacy of linagliptin as add-on therapy to metformin in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled study.
Diabetes Obes Metab 2011; 13: 65–74.
11. Owens DR, Swallow R, Dugi KA, Woer le HJ. Efficacy and safety of linagliptin in persons with type 2 diabetes inadequately controlled by a combination of metformin and sulphonylurea: a 24-week randomized study. Diabet Med 2011; 28: 1352–61.
12. Gallwitz B, Rosenstock J, Rauch T, et al. 2-year efficacy and safety of linagliptin compared with glimepiride in patients with type 2 diabetes inadequately controlled on metformin: a randomised, double-blind, non-inferiority trial. Lancet 2012; 380: 475–83.