PCSK9 levels altered by simvastin, but not ezetimibe treatment
11/04/2013
Changes in PCSK9 levels are affected by decreasing LDL-C levels and PCSK9 baseline levels.
Evidence from a Randomized Trial That Simvastatin, but Not Ezetimibe, Upregulates Circulating PCSK9 Levels.Literature - Berthold HK, Seidah NG, Benjannet S, and Gouni-Berthold I. - PLoS One. 2013;8(3):e60095. doi: 10.1371/journal.pone.0060095. Epub 2013 Mar 27.
Berthold HK, Seidah NG, Benjannet S, and Gouni-Berthold I.
PLoS One. 2013;8(3):e60095. doi: 10.1371/journal.pone.0060095. Epub 2013 Mar 27.
Background
Statins not only lower LDL-C levels, but also upregulate LDL-receptor (LDL-R) and Proprotein convertase subtilisin/kexin type 9 (PCSK9) protein [1]. PCSK9 is a protein that binds the LDLR and targets it for degradation [2]. Upregulation of PCSK9 could inhibit the beneficial effects of statins [3,4] and PCSK9 concentrations have been associated with the response to statins [5]. This suggests a physiologically and clinically relevant function of circulating PCSK9.It is therefore interesting to study how lipid-modifying pharmacological agents affect PCSK9 concentrations. Very few data exist on the effects of ezetimibe (alone or combined with a statin) on PCSK9 levels [5]. It is furthermore unclear which other parameters might influence changes in PCSK9 concentrations during lipid-lowering therapy.
This randomised study therefore aimed to investigate the effect of ezetimibe alone or in combination with simvastatin, on circulating PCSK9 levels.
Main results
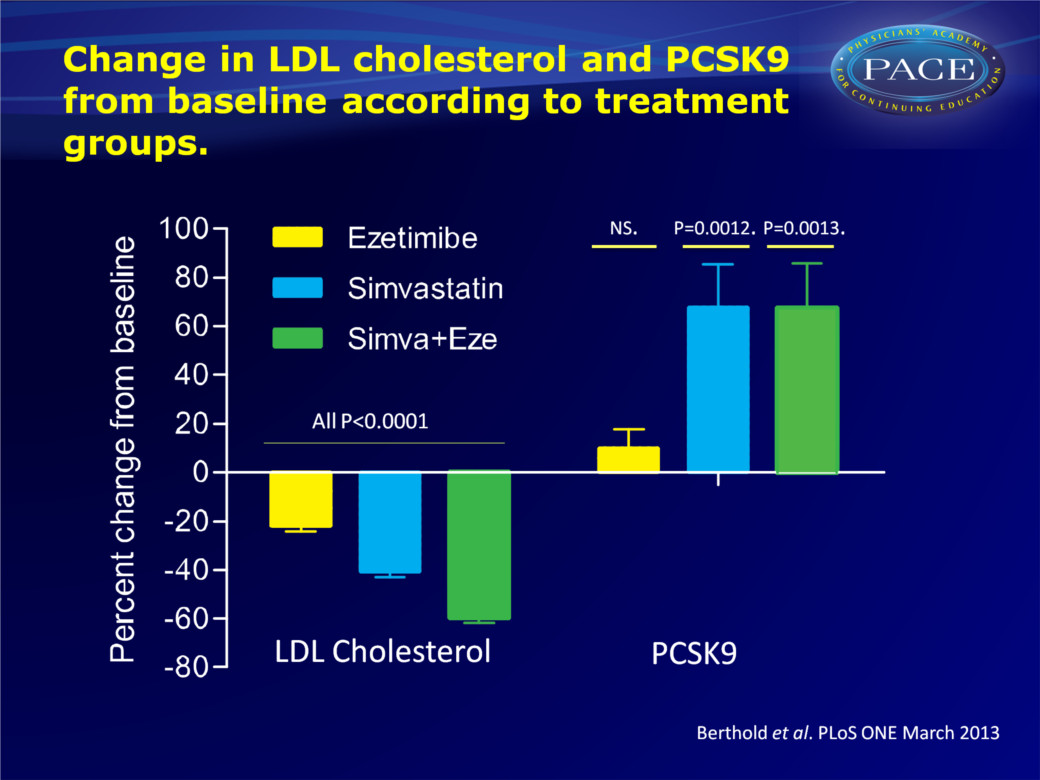
- LDL-C decreased by 22% in patients treated with ezetimibe, 41% after simvastatin and 60% in the simvastatin+ezetimibe group.
- PCSK9 concentrations increased with 9.9 + 38% (not statistically significant) in the ezetimibe-treated group, with 67.8 + 85.2% (P=0.0012) in the simvastatin group and 67.3 + 90.7% (P=0.0013) in the group receiving combined treatment.
- Baseline PCSK9 concentrations (β=-1.68, t=-4.04, P<0.001) and the percent change in LDL-C from baseline (β=1.94, t=2.52, P=0.014) had a statistically significant effect on change in PCSK9 concentrations.
- Subjects with low baseline PCSK9 (<40 ng/ml) showed the strongest increase in plasma PCSK9 levels, as well as a pronounced LDL-C-lowering effect (>50% from baseline) under treatment. PCSK9 hardly changed in subjects with high baseline PCSK9 concentrations (>60 ng/ml), even in the presence of pronounced LDL-C lowering.
- Subjects with low baseline PCSK9 (<40 ng/ml) and moderate LDL-C decrease (30-50% from baseline) showed robust upregulation of PCSK9 levels.
- Significant changes in PCSK9 by lipid-lowering medication were only seen after simvastatin treatment (with or without ezetimibe), but not under ezetimibe alone.
Conclusion
Changes in PCSK9 concentration are mostly affected by and seem tightly regulated by the decrease in LDL-C levels and by baseline PCSK9. Thus, genetic variations in PCSK9 are at play. Only simvastatin significantly influenced PCSK9 levels; ezetimibe monotherapy did not. The increase in PCSK9 levels after standard simvastatin treatment (40 mg/d) was not further enhanced after addition of ezetimibe, despite its LDL-C-lowering effect. These findings may help identify individuals who would benefit most from treatment with PCSK9 antibodies, currently under development. The results need to be confirmed in other, larger studies.Download PPT
References
1.Tibolla G, Norata GD, Artali R, et al. (2011) Proprotein convertase subtilisin/kexin type 9 (PCSK9): from structure-function relation to therapeutic inhibition. Nutr Metab Cardiovasc Dis 21: 835–843.2.Seidah NG, Prat A (2012) The biology and therapeutic targeting of the proprotein convertases. Nat Rev Drug Discov 11: 367–383.
3. Careskey HE, Davis RA, Alborn WE, et al. (2008) Atorvastatin increases human serum levels of proprotein convertase subtilisin/kexin type 9. J Lipid Res 49: 394–398.
4.. Seidah NG (2009) PCSK9 as a therapeutic target of dyslipidemia. Expert Opin Ther Targets 13: 19–28.
5. Konrad RJ, Troutt JS, Cao G (2011) Effects of currently prescribed LDL-C lowering drugs on PCSK9 and implications for the next generation of LDL-C lowering agents. Lipids Health Dis 10: 38. 1476-511.
Find this article on Pubmed